132IoT Use Cases: Medication Adherence and Chronic Disease
132.1 Medication Adherence: The Hidden Healthcare Crisis
Time: ~12 min | Level: Intermediate | Unit: P03.C03.U08
132.2 Learning Objectives
By the end of this section, you will be able to:
Quantify the medication adherence crisis and its economic impact
Design IoT solutions for medication adherence improvement
Understand ingestible sensor technology for verification
Analyze EHR integration challenges in healthcare IoT
Apply worked examples to real-world compliance scenarios
ImportantThe Medication Adherence Crisis: A $300 Billion Problem
The Scale of Non-Adherence:
Statistic
Value
Source
US healthcare spending on chronic conditions
84% of total
Johns Hopkins University
Prescribed medications NOT taken as directed
>50%
WHO
Annual US cost of non-adherence
$100-300 billion
NEHI
Hospital admissions due to non-adherence
10-25%
Multiple studies
Why People Don’t Take Their Medications:
Barrier
IoT Solution
Forgetfulness
Smart dispensers with alerts, wearable reminders
Uncertainty about effectiveness
Connected monitoring showing health improvements
Fear of side effects
Real-time tracking to catch adverse reactions early
Difficulty with regimen complexity
Automated sorting, timing, and dosing
Cost concerns
Data proving value leads to insurance coverage justification
132.3 Smart Medication Dispenser Architecture
Medication Adherence Device
Figure 132.1: Medication adherence device showing connected pill dispenser with scheduling, reminders, compliance tracking, and caregiver notifications.
Smart Pill Dispenser IoT Architecture:
Flowchart diagram
Figure 132.2: Smart medication adherence system architecture showing pill dispenser with sensors, connectivity to cloud platform, and multi-stakeholder notification chain.
Key System Components:
Component
Function
Technology
Pill Compartments
Store medications by time/day
RFID-tagged trays, weight sensors
Dispensing Mechanism
Control access to correct pills
Locked compartments, motor-driven carousel
Reminder System
Alert patient when dose due
Audio/visual alarms, phone notifications
Verification Sensors
Confirm pill removal
Light beam break, weight change, camera
Connectivity
Report to cloud
Wi-Fi, cellular, or LoRaWAN
Backup
Operate during outages
Local storage, battery, offline operation
132.4 Ingestible Sensors: The Next Frontier
The most advanced IoT approach to adherence verification uses ingestible sensors that confirm actual medication consumption:
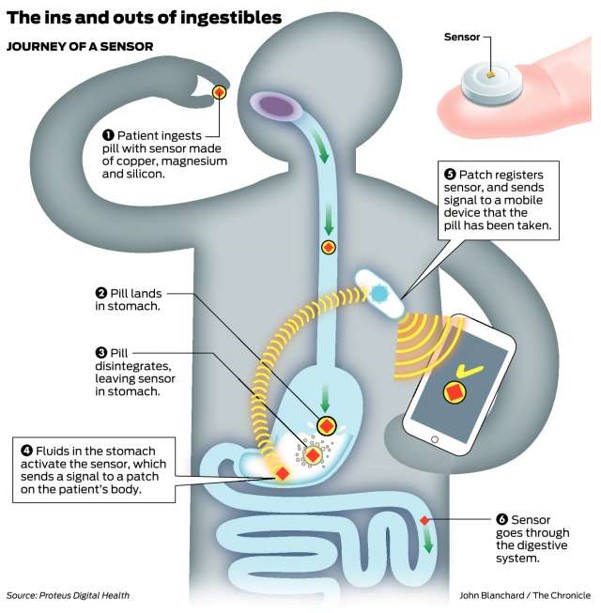
Proteus Digital Health System Architecture:
Flowchart diagram
Figure 132.3: Ingestible sensor system: Smart pill with embedded sensor dissolves in stomach, stomach acid powers the sensor, signal transmits through body tissue to wearable patch, patch relays data via Bluetooth to smartphone, cloud platform provides verified adherence data to healthcare providers.
How the Ingestible Sensor Works:
The Sensor: A 1mm chip made of copper, magnesium, and silicon - edible materials already in multivitamins
Power Source: Stomach acid acts as electrolyte, creating a tiny battery (~1 volt) when pill dissolves
Signal Transmission: Low-power signal travels through body tissue to wearable patch
Data Chain: Patch to Smartphone to Cloud to Healthcare provider dashboard
Outcome: Irrefutable proof of ingestion with precise timestamp
Why This Matters for Chronic Disease:
Clinical trials: Verify actual drug exposure, not just dispensing
Insurance: Value-based contracts tied to proven adherence
High-stakes medications: Transplant anti-rejection drugs, HIV antiretrovirals, psychiatric medications
Opioid monitoring: Verify appropriate use in pain management
Privacy Considerations: The ability to track exact medication ingestion raises significant privacy concerns. Systems must balance clinical benefit against surveillance risks, with clear patient consent and data ownership policies.
132.5 Chronic Disease Monitoring: The Parkinson’s Challenge
WarningChronic Disease Monitoring: Why Continuous Data Matters
The Problem with Periodic Checkups:
Patients with chronic neurological conditions like Parkinson’s disease experience daily symptom fluctuations that monthly doctor visits cannot capture. By the time a patient sees their neurologist, the “good days” and “bad days” have averaged out, making medication optimization nearly impossible.
The Scale of Parkinson’s Disease:
Statistic
Value
Implication for IoT
Prevalence over 60
1 in 100
Massive addressable market
US patients
1 million
Need for scalable monitoring
Worldwide patients
5+ million
Global healthcare burden
New diagnoses/year
60,000 (US)
Growing demand
Dopamine cells lost at diagnosis
60-80%
Early detection crucial
Why IoT Changes Everything:
Traditional model: 30 minutes/month of clinical observation IoT model: 43,200 minutes/month of continuous data (24/7)
Key IoT Biomarkers for Parkinson’s:
Biomarker
Sensor
What It Reveals
Tremor frequency
3-axis accelerometer
Symptom severity (4-6 Hz = PD tremor)
Gait pattern
IMU + GPS
Freezing episodes, shuffling
Voice quality
Microphone
Hypophonia, monotone speech
Typing rhythm
Touchscreen
Fine motor control degradation
Sleep movement
Bed sensor
REM sleep behavior disorder
The mPower App: Smartphone as Medical Device
The Parkinson’s mPower app demonstrates how smartphones become clinical assessment tools:
Test
What It Measures
Clinical Insight
Spatial Memory Test
Pattern recall and repetition
Cognitive decline tracking
Tapping Interval Test
Finger tap speed and rhythm
Bradykinesia (slowness of movement)
Voice Test
Sustained “Aaaah” phonation
Hypophonia, vocal tremor, breath control
Walking Test
Gait via accelerometer
Shuffling, freezing episodes
The Active vs. Passive Monitoring Paradigm:
“Instead of patients actively performing certain tasks, could we monitor disease progression passively in the background?”
This is the holy grail of digital health - moving from active tests (patient must remember to do them) to passive monitoring (continuous background sensing). Passive monitoring captures real-world behavior, not artificial test conditions.
132.6 Healthcare IoT’s Biggest Barrier: EHR Integration
The Integration Gap:
Despite the promise of consumer health wearables and IoT medical devices, lack of Electronic Health Record (EHR) integration remains the primary barrier to clinical adoption. A device that doesn’t flow data into the patient’s medical record is, from a clinical workflow perspective, invisible.
TipMVU: Healthcare IoT Regulatory Compliance
Core Concept: Healthcare IoT devices must navigate a regulatory triad: FDA clearance for device safety and efficacy, HIPAA compliance for data privacy and security, and HL7/FHIR standards for clinical system interoperability. Why It Matters: A brilliant health sensor that cannot integrate with Electronic Health Records (EHRs) is clinically invisible - physicians cannot see the data during patient encounters. Devices without FDA clearance cannot make diagnostic claims, limiting reimbursement options. HIPAA violations carry penalties up to $1.5M per incident category per year. Key Takeaway: Design healthcare IoT “integration-first” - a simple device with EHR connectivity via FHIR APIs delivers more clinical value than a sophisticated sensor that creates another data silo. Budget 6-18 months and 30-40% of development costs for regulatory compliance before market launch.
The “Integration-First” Mindset:
“Sometimes, a dumb gadget can be as useful as a smart one if it could integrate seamlessly with the EHR.”
This counterintuitive insight reveals a key failure mode in healthcare IoT:
Approach
Result
Cool gadget, no integration
Consumer curiosity leads to abandonment in 3 months
Simple device, EHR integration
Clinical workflow adoption leads to long-term use
Why EHR Integration Is Hard:
Legacy systems: Most EHRs (Epic, Cerner, Meditech) are 20+ year old architectures
Regulatory burden: FDA clearance, HIPAA compliance, clinical validation
Data standards fragmentation: HL7v2, FHIR, proprietary APIs
Business models: EHR vendors charge for integration, creating barriers
Liability concerns: Who’s responsible if IoT data leads to missed diagnosis?
The FHIR Standard: A Path Forward
FHIR (Fast Healthcare Interoperability Resources) is emerging as the API standard for healthcare data exchange:
RESTful architecture: Modern web-friendly APIs
Standardized resources: Patient, Observation, Device defined schemas
Mandated adoption: US 21st Century Cures Act requires FHIR support
Apple HealthKit: Now exports to FHIR-enabled EHRs
Design Implication: When designing healthcare IoT, start with the EHR integration architecture, not the sensor. The question isn’t “what can we measure?” but “what can we get into the clinical record?”
132.7 Worked Example: Remote Patient Monitoring HIPAA Compliance
Scenario: A regional health system is deploying a Remote Patient Monitoring (RPM) program for 2,000 heart failure patients to qualify for CMS reimbursement codes (CPT 99453-99458). The system must achieve full HIPAA compliance while integrating with Epic EHR.
Given: - Patient devices: Bluetooth-enabled weight scale, blood pressure cuff, pulse oximeter - Data transmission: Cellular gateway in patient home to cloud platform - EHR integration: Epic MyChart patient portal + provider dashboard via FHIR R4 API - HIPAA requirements: PHI encryption at rest (AES-256) and in transit (TLS 1.3) - CMS RPM billing requirements: Minimum 16 days of data transmission per 30-day period - Patient population: Average age 68, 40% have limited smartphone proficiency - Budget: $150/patient/month all-in (device, connectivity, software, support)
Steps:
Map PHI data flows and identify HIPAA touchpoints:
Device to gateway: BLE with encrypted pairing (no PHI in transit - device ID only)
Gateway to cloud: Cellular with TLS 1.3 (PHI: vital signs + patient ID)
FHIR Device resource: Link observations to specific patient device
Clinical workflow: Abnormal readings trigger Epic In-Basket message to care team
Patient engagement: MyChart displays daily readings and trend graphs
Validate CMS billing compliance:
CPT 99453: Initial setup and patient education ($19.19 reimbursement)
CPT 99454: Device supply with daily recordings, 16+ days/month ($55.72/month)
CPT 99457: 20+ minutes clinical staff time ($48.80/month)
CPT 99458: Additional 20 minutes ($40.42/month)
Maximum monthly reimbursement per patient: $144.94
Result: System achieves HIPAA compliance with documented Business Associate Agreements covering 3 vendors, passes SOC 2 Type II audit, and integrates bidirectionally with Epic. Average patient achieves 22 transmission days/month, qualifying for full CMS reimbursement. Net margin: $144.94 - $150 = -$5.06/patient/month before reduced hospitalization savings.
Key Insight: Healthcare IoT economics often depend more on regulatory compliance and reimbursement qualification than on technology costs. The $4/month HIPAA overhead and EHR integration complexity represent invisible costs that consumer IoT companies underestimate when entering healthcare markets.
132.8 Worked Example: Continuous Glucose Monitor Data Accuracy
Scenario: A diabetes management app integrates data from continuous glucose monitors (CGMs) to provide insulin dosing recommendations. The system must validate sensor accuracy and handle calibration drift.
Given: - CGM sensor: Abbott FreeStyle Libre 3 (14-day wear, factory calibrated) - Published MARD (Mean Absolute Relative Difference): 7.8% - Target glucose range: 70-180 mg/dL - Insulin sensitivity factor: 1 unit lowers blood glucose by 50 mg/dL - Critical thresholds: <54 mg/dL (severe hypoglycemia), >250 mg/dL (hyperglycemia) - Patient population: Type 1 diabetics with 4-6 insulin injections daily - Decision support requirement: Recommend corrections within +/- 0.5 units
Steps:
Quantify accuracy impact on dosing decisions:
At 150 mg/dL true glucose, 7.8% MARD means readings range 138-162 mg/dL
12 mg/dL variation translates to 0.24 units dosing variation (12 / 50)
This is within +/- 0.5 unit target for most readings
Identify high-risk accuracy scenarios:
First 24 hours after sensor insertion: MARD increases to 12-15%
Rapid glucose changes (>2 mg/dL/min): Lag creates 15-20 min delay
Compression lows: Lying on sensor causes false low readings
End of sensor life (days 12-14): Accuracy degradation observed
Design calibration validation logic:
Require fingerstick confirmation for readings <70 or >250 mg/dL
Flag readings during first 12 hours as “warming up”
Detect rapid change rate and apply trend arrows, not absolute values
Compare consecutive readings to detect sensor drift (>20 mg/dL jump)
Critical high (250 mg/dL): Apply 10% buffer, alert at 225 mg/dL
Dosing decisions: Require 2 consecutive readings within 10% to act
Implement decision support guardrails:
Maximum single correction: 4 units (regardless of calculation)
Minimum time between corrections: 3 hours (insulin action duration)
Stacking prevention: Display active insulin on board (IOB)
Result: Decision support system provides recommendations within +/- 0.5 units for 94% of scenarios, with mandatory fingerstick confirmation for 6% edge cases. Time in range (70-180 mg/dL) improves from 55% to 68% for pilot users.
Key Insight: Healthcare IoT systems must design around sensor limitations, not assume perfect accuracy. CGM MARD of 7.8% sounds small but translates to clinically significant dosing variations at glucose extremes. Safety-critical systems require multiple validation layers and clear user guidance on when automated recommendations should not be trusted.
132.9 Knowledge Check
Show code
{const container =document.getElementById('kc-usecase-medication');if (container &&typeof InlineKnowledgeCheck !=='undefined') { container.innerHTML=''; container.appendChild(InlineKnowledgeCheck.create({question:"A healthcare startup is developing an IoT medication adherence system. They have a choice between (A) a sophisticated smart pill bottle with 15 sensors and AI-powered predictions but no EHR integration, or (B) a simple bottle with a single weight sensor that integrates with Epic EHR via FHIR. Which approach is more likely to achieve clinical adoption?",options: [ {text:"Option A - More sensors means better data and clinical value",correct:false,feedback:"More sensors don't translate to clinical value if physicians never see the data. A device invisible to clinical workflows has zero impact on care decisions, regardless of its technical sophistication."}, {text:"Option B - EHR integration trumps sensor sophistication for clinical adoption",correct:true,feedback:"Correct! The integration-first insight is counterintuitive but proven: a simple device with EHR connectivity delivers more clinical value than a sophisticated sensor creating another data silo. Physicians make decisions based on data in the EHR - data that never reaches the clinical record might as well not exist. Budget 30-40% of development for integration, not more sensors."}, {text:"Both are equivalent - success depends on marketing and user experience",correct:false,feedback:"Clinical adoption is driven by workflow integration, not marketing. A device that surfaces data in the physician's existing workflow (EHR) will see adoption; one requiring a separate login and dashboard will be ignored regardless of UX quality."}, {text:"Cannot determine without knowing the specific medication and patient population",correct:false,feedback:"While context matters, the EHR integration principle applies universally. Any medication adherence data invisible to the prescribing physician has no mechanism to improve care. This is a fundamental healthcare IoT design principle."} ],difficulty:"medium",topic:"iot-use-cases-medication" })); }}